
Dr. Muneeb Ullah – Expert Surgeon in Islamabad, Pakistan
Abstract
Gallbladder stones impacted at neck of gallbladder can result in acute calculous cholecystitis with mucocele gallbladder. Laparoscopic cholecystectomy is performed in such cases as an emergency surgery. We present a case long gallbladder with mucocele formation that was managed by laparoscopic approach. The gallbladder removed was 27.8cm in length. This is the longest gallbladder removed by laparoscopic cholecystectomy in Pakistan so far. The patient had uneventful recovery.
Introduction
Diseases of gallbladder have a wide spectrum that includes asymptomatic gallstones, biliary colic, cholecystitis, mucocele, empyema gallbladder, gangrene, perforation, peritonitis, polyps and malignancy.1 The definitive treatment warrants surgical intervention in the form of laparoscopic or open cholecystectomy.2 One of the emergency presentations is acute calculous cholecystitis which, if associated with gallstone impacted at neck, would require emergency surgery.3 This impaction can also result in over-distended mucocele gallbladder or empyema gallbladder. Laparoscopic cholecystectomy is performed in routine, for such patients with aim to minimize the trauma without compromising the efficacy of the treatment. It also leads to lesser pain, shorter hospital stay and early return to routine activity.4 We present a case of overdistended huge mucocele of gallbladder secondary to acute calculous cholecystitis successfully managed by laparoscopic cholecystectomy at Maroof International Hospital, Islamabad.
Case Presentation
Our patient was a 45 years old female who presented with pain in right upper quadrant of abdomen with nausea for the last six days. It was sudden and started after she had a pizza with cheese topping. There was no vomiting, anorexia or fever. The pain remained constant with bouts in between and some decrease in intensity with oral analgesics. There was no pruritis, discoloration of eyes, dark urine or clay-colored stools. She initially went to a general physician who then referred the patient to us. On examination, the patient had tender right hypochondrium with positive murphy’s sign and a palpable gallbladder. While the liver function tests were normal, the hepatobiliary ultrasound reported a solitary 12mm stone impacted in the neck of overdistended gallbladder as well as increased gallbladder wall thickness of 4.5mm. The patient was planned for laparoscopic cholecystectomy in acute calculous cholecystitis. Standard four ports were used. Diagnostic laparoscopy revealed acutely inflamed overdistended gallbladder (Figure 1 and 2).
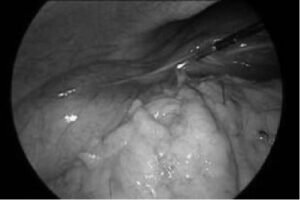
Figure 1: Peroperative image of gallbladder

Figure 2: Peroperative image of gallbladder.
Gallbladder contents were aspirated using aspiration needle that revealed mucocele gallbladder. Afterwards laparoscopic cholecystectomy was completed. The size of gallbladder (postoperative) was 27.8cm (Figure 3)

Figure 3: Postoperative image of Gallbladder
Patient was discharged the next day. Follow up consultations revealed uneventful recovery.
Discussion
Gallbladder is situated on the undersurface of segment IV and V of liver and has a peritoneal attachment to liver.5 The critical knowledge of anatomy, its variations and clinical experience is necessary for a safe and uneventful surgery.3 The gallbladder is a pear shaped organ with an average length of 4.5 to11.6 cm and capacity of 30 to 50ml.6 Acute calculous cholecystitis is accompanied by inflammation of gallbladder that presents as a combination of right upper quadrant pain that may radiate to the back or right shoulder, nausea, vomiting and fever.7 In cases where the gallbladder stone is impacted at the neck of gallbladder, cystic duct is blocked that results in the mucus accumulation within the gallbladder. This leads to over distended gallbladder i.e. mucocele.8 Prolonged obstruction of cystic duct leads to continuous mucin secretion that ultimately overdistends the gallbladder causing gallbladder wall edema, dilation, inflammation, infection or perforation. In patients with diabetes mellitus especially who have poor control, there is autonomic neuropathy and cholecystoparesis that causes cholecystomegaly.6 In our case, stone impacted at neck caused overdistension of gallbladder. Mucocele itself is not an infective pathology but if bacterial contamination occurs, it can lead to empyema gallbladder.9 Empyema gallbladder and mucocele are emergency pathologies that require early intervention in the form of laparoscopic cholecystectomy unless there is some definitive contraindication. The advantage of laparoscopy in such cases is that, it yields minimal scar, less pain and early mobilization. The huge sized or overdistended gallbladders are attributed to congenital anomalies, acquired or obstructive causes as per literature review.10 Previously, in Pakistan, the largest gallbladder removed via laparoscopic cholecystectomy was 25.5cm at capital hospital Islamabad as reported by Taj N et al. 6 Currently the largest gallbladder removed laparoscopically by laparoscopic cholecystectomy is 30cm.3 In our case the length of the gallbladder was 27.8cm which is the longest documented gallbladder removed laparoscopically so far in Pakistan to date. This case report shows that apart from pathological variation, laparoscopic cholecystectomy is still the choice for operating acute or mucocele gallbladders. Patient mobilizes early and is discharged as per routine and large scars can be avoided.
Conclusion
Huge gallbladders, although difficult to handle but can safely be removed via laparoscopic cholecystectomy with good outcomes. A sound knowledge of gallbladder anatomy, experience of surgeon and good team are corner stones in such surgeries.

